When you experience a sudden, sharp pain in your shoulder following a fall or an accident, the possibility of a fractured shoulder becomes a reality. A shoulder fracture can immediately impact your ability to perform daily tasks. In this post, we’ll discuss the nature of a fractured shoulder, the diagnostic process, the range of treatment options available, and the path to recovery.
Key Takeaways
- Fractures may occur in the proximal humerus (upper arm bone), clavicle (collarbone), or rarely, the scapula (shoulder blade).
- A thorough physical examination and imaging tests are frequently used to classify the fracture and determine the best course of action.
- The decision between non-surgical management (sling immobilization) and surgical intervention (fixation or replacement) depends heavily on the type of fracture, the degree of displacement, and your overall health and activity level.
The Anatomy of a Fractured Shoulder
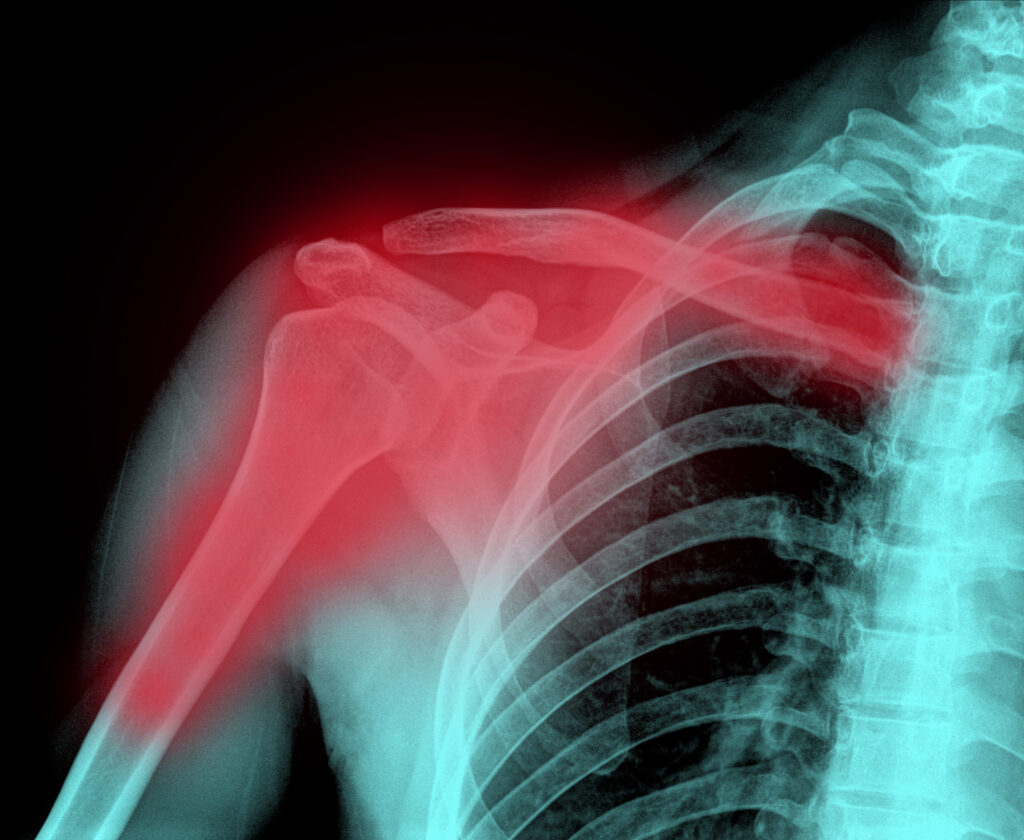
The shoulder is the most mobile joint in the human body, a complex structure composed of three main bones: the humerus, the clavicle, and the scapula.
- The Humerus (Upper Arm Bone): The top part of the humerus, known as the proximal humerus, forms the “ball” of the ball-and-socket joint. Fractures in the proximal humerus are common, especially in older adults with osteoporosis.
- The Clavicle (Collarbone): This long, slender bone connects the shoulder blade to the sternum (breastbone). Clavicle fractures are especially prevalent in athletes and younger individuals, often resulting from a direct blow or a fall.
- The Scapula (Shoulder Blade): The scapula is a large, flat, triangular bone that forms the “socket” (glenoid) of the joint. Scapular fractures are relatively rare. They usually require a significant amount of force, suggesting a high-energy trauma like a motor vehicle accident.
Understanding Fracture Types
Fractures are generally classified based on how the bone fragments line up. A non-displaced fracture means the bone has broken, but the pieces remain in their correct anatomical position. In contrast, a displaced fracture occurs when the bone fragments shift out of alignment. If the displacement is significant, the bone may not heal correctly on its own and surgical intervention may be required to restore normal structure. An open (or compound) fracture involves a break where the bone pierces through the skin, creating an open wound.
Recognizing the Signs: Diagnosis of a Fractured Shoulder
The onset of a shoulder fracture is typically marked by several signs:
- Severe Pain: You may feel intense pain that worsens with any attempt to move the arm or shoulder.
- Swelling and Bruising: Swelling around the shoulder joint and the upper arm is common. Bruising may develop quickly and can spread down the arm and even to the chest.
- Inability to Move: You will likely find it extremely painful to lift or rotate your arm. In some cases, any movement may cause a grinding sensation, known as crepitus.
- Deformity: In cases of a severely displaced fracture, the shoulder may appear visibly deformed or “out of place.”
The Diagnostic Process
Diagnosis is the first step toward proper treatment. Your doctor will generally begin with a physical examination, checking your shoulder, arm, and hand for tenderness, swelling, bruising, and any signs of nerve or blood vessel damage.
Imaging studies may be used to confirm the fracture. X-rays are typically taken from several angles to clearly show the injury and determine the fracture type. If the break is complex, especially near the joint or if the bone is severely displaced, a CT scan may be ordered for a more detailed, three-dimensional view. This can be especially helpful when planning surgery.
Treatment Options: Non-Surgical vs. Surgical Approaches
The treatment for a fractured shoulder is typically dependent on the location and severity of the break. Some shoulder fractures, particularly those that are non-displaced, can be managed without surgery. However, more complex injuries may require surgical intervention to achieve a stable and functional result.
Non-Surgical Management
Non-surgical treatment is the preferred approach for the majority of clavicle fractures, most scapular fractures, and many non-displaced proximal humerus fractures.
- Immobilization: Immobilizing the fracture site may allow the bone to heal. This is typically achieved using a sling or a specialized shoulder immobilizer. Patients wear this device for a specific period of time depending on the severity and type of fracture.
- Pain Management: Pain medication may be used to manage discomfort. Ice application is also a simple way to help reduce swelling and pain, especially in the first few days.
- Early Gentle Motion: While the fracture needs time to heal, prolonged immobilization can lead to shoulder stiffness. Your doctor may recommend very gentle, passive range-of-motion exercises, such as pendulum exercises, to begin soon after the injury.
- Monitoring: You may have follow-up appointments, often including repeat X-rays, to ensure the fracture fragments are maintaining their position and healing properly.
Surgical Intervention
Surgery may become necessary when the fracture is displaced, unstable, or involves the joint surface in a way that non-surgical treatment cannot correct. The goal of surgery is to restore the normal anatomy of the shoulder, stabilize the bone fragments, and allow for earlier, safer rehabilitation. An experienced orthopedic surgeon can evaluate the fracture and recommend the best surgical approach.
1. Open Reduction and Internal Fixation (ORIF)
This procedure is commonly used for displaced clavicle fractures and certain proximal humerus fractures.
- Open Reduction: The surgeon makes an incision to access the fracture site and manually realigns the bone fragments back into their correct anatomical position.
- Internal Fixation: Once aligned, the fragments are held securely in place using specialized orthopedic hardware.
2. Shoulder Replacement (Arthroplasty)
In cases where the fracture is so severe that the blood supply to the humeral head is compromised, or the bone is shattered into too many pieces to be fixed, a shoulder replacement may be the recommended option:
- Total Shoulder Arthroplasty: Both the ball and the socket are replaced with prosthetic components.
- Reverse Total Shoulder Arthroplasty: This is a specialized procedure where the ball and socket components are reversed. The ball is placed on the shoulder blade (scapula), and the socket is placed on the upper arm bone (humerus). This design is often preferred for fracture cases, especially in older patients, because it relies on the deltoid muscle rather than the damaged rotator cuff to power the arm’s movement.
Your surgeon will discuss the risks, benefits, and expected outcomes of each option based on your specific fracture pattern, age, and functional demands.
Preventing Shoulder Fractures
Understanding the risk factors and taking proactive steps may help reduce your chances of a future injury.
Risk Factors for Shoulder Fractures
Certain factors can increase your susceptibility to a shoulder fracture:
- Osteoporosis: This condition causes bones to become weak and brittle. It is a risk factor for low-energy fractures, such as a fall from a standing height, particularly in the proximal humerus.
- Age: As people age, bone density naturally decreases, and the risk of falling increases.
- Participation in High-Impact Sports: Activities like skiing, football, and cycling carry a higher risk of direct trauma to the shoulder or falls that can result in a clavicle or scapular fracture.
- Poor Balance and Coordination: Conditions that affect balance can increase the likelihood of a fall.
Prevention Strategies
You can take concrete steps to protect your bone health and reduce your risk of a fall.
- Bone Health: Discuss bone density testing and supplementation with your doctor.
- Fall Prevention: Modify your home environment to reduce tripping hazards. This includes securing loose rugs, improving lighting, and installing grab bars in bathrooms.
- Protective Gear: Always wear appropriate protective equipment, such as shoulder pads or wrist guards, when participating in high-risk sports.
Summary
A fractured shoulder is an injury that may require timely diagnosis, individualized treatment, and guided rehabilitation. Whether managed with immobilization or surgical intervention, the treatment approach depends on factors such as fracture type, displacement, and patient-specific needs. Recovery frequently involves a combination of physical therapy, activity modification, and follow-up imaging to ensure appropriate healing. While recovery timelines vary, adherence to medical guidance and a consistent rehabilitation effort can support meaningful improvements in strength, mobility, and quality of life.
Frequently Asked Questions
How long does it take for a fractured shoulder to heal?
The initial bone healing for most shoulder fractures, such as a non-displaced proximal humerus fracture, typically takes around six to eight weeks. However, this is only the beginning of the recovery process. Regaining strength and range of motion through physical therapy may take anywhere from three to six months, and sometimes longer for complex injuries or surgical cases.
Will I need surgery for my fractured shoulder?
Many shoulder fractures do not require surgery. Non-displaced fractures, where the bone pieces are still well-aligned, are often treated successfully with a sling and physical therapy. Surgery is generally reserved for fractures that are displaced, unstable, involve the joint surface, or have a high risk of complications.
Can I sleep on my side with a fractured shoulder?
In the early stages of healing, sleeping on the fractured side is usually difficult due to pain. Even sleeping on the non-fractured side can be uncomfortable because the weight of your body can pull on the injured shoulder. Many patients find the most comfort sleeping in a semi-reclined position. Consider a recliner chair or being propped up in bed with several pillows. Follow your doctor’s specific instructions regarding positioning and sling use while sleeping.



